Underpayments are among the most overlooked revenue issues in behavioral health billing. They do not scream for attention as denials do. They sit quietly in the system. Most practices see a paid claim and move on. That is where the money slips away.
Behavioral health claims are especially vulnerable to underpayments. Therapy services are time-based. Psychiatry codes have strict documentation rules. Add-on codes get missed often. Payers know this. They rely on practices that do not check deeply. That is the harsh truth.
Underpaid behavioral health insurance claims are more common than most providers realize, and many mental health billing services overlook them entirely.
When underpayments go unappealed, revenue slowly bleeds out. Month after month. Year after year. Practices then blame low reimbursement rates, while the real issue stays hidden.
Appealing underpayments is not aggressive billing. It is compliant billing. You are simply asking to be paid what the contract already allows.
Why Underpayments Happen in Behavioral Health
Underpayments happen in behavioral health more often than most practices realize. The work is complex. The rules are strict. Payers rely heavily on automated systems. Small gaps lead to reduced payment. The claim still shows as paid. That is why the issue stays hidden.
- One primary reason is time-based coding. Behavioral health relies on time more than many other specialties. Therapy codes change based on minutes. Crisis services extend beyond base time. When documentation does not clearly state the total time, payer systems downgrade the code. A 60-minute session gets paid like a 45-minute session. The payer saves money. The practice loses revenue.
- Another common cause is the omission of add-on codes. Codes like crisis add-ons or prolonged services must be linked correctly to the primary service. If the payer system fails to recognize that link, the add-on gets stripped. No denial appears. Payment posts lower than expected. Many practices assume the add-on was non-covered. In reality, it was processed incorrectly.
- Modifier misprocessing is another frequent problem. Behavioral health claims often require modifiers like 25, 59, or telehealth modifiers. Even when applied correctly, payer systems may treat them as bundled services. This leads to reduced payment. The EOB rarely explains the reduction clearly. Without manual review, the underpayment goes unnoticed.
- Provider credential issues also drive underpayments. Psychiatrists, psychologists, LCSWs, and LPCs all have different reimbursement rules. When a payer processes a psychiatrist’s claim at a therapist rate, payment drops significantly. This usually happens due to credential file errors on the payer side. Practices assume the rate is correct. It is not.
- Parity law misapplication also plays a quiet role. Behavioral health parity laws require equal treatment compared to medical services. Many payers still fail to apply parity correctly. They cap rates. They reduce session reimbursement. They use outdated limits. These errors show up as underpayments rather than denials.
- Telehealth processing errors have increased underpayments in recent years. Incorrect place-of-service codes or missing modifiers often result in reduced payment. Even when telehealth is covered, payer systems may default to lower in-person rates or deny add-on payments due to logic. The claim pays partially. The problem stays buried.
- Outdated fee schedules also cause underpayments. Payers sometimes apply older contract rates. Fee schedules change. Practices rarely verify allowed amounts after updates. When the allowed amount is incorrect, the payment is wrong. Without contract comparison, the error stands.
The Financial Impact of Ignoring Underpaid Claims
Ignoring underpaid claims creates a slow and steady drain on mental health practices. The damage does not show up overnight. It builds quietly over time. Most providers focus on denials and no-pay claims. Underpayments slip through because the claim shows as paid. That small assumption costs real money.
- Mental health services are often high-volume and time-based. Therapy sessions happen daily. Psychiatry visits are repeated weekly. When each encounter is underpaid by a small amount, the loss multiplies fast. Ten or twenty dollars per session does not feel significant at first. Across hundreds of sessions each month, the impact becomes serious.
- Revenue leakage from underpayments directly affects cash flow. Practices assume their payer rates are low when, in reality, the payer is not paying correctly. This creates a false picture of financial performance. Providers may see full schedules but still struggle to meet revenue goals. The problem is not demand. It is payment accuracy.
- Underpayments also distort productivity metrics. Providers appear less profitable than they genuinely are. Administrators may reduce hours, delay hiring, or limit services based on inaccurate data. All of this happens because earned revenue was never recovered.
- Over time, ignoring underpayments weakens negotiating power with payers. When renewal discussions come up, practices rely on reported collections. If collections are artificially low due to underpayments, leverage is lost. The payer controls the narrative. The provider accepts unfavorable terms without realizing it.
- Mental health practices also absorb higher administrative costs when underpayments go unchecked. Staff spend time reconciling accounts that are never truly balanced. Financial planning becomes reactive. Budgeting becomes uncertain. Stress increases across the organization.
- Mental health providers lose between 3 percent and 7 percent of annual revenue due to underpayments alone. For a small practice, this could mean thousands each year. For larger groups, the loss can reach six figures. This revenue was already earned. It was not claimed.
Appeal Deadlines and Timely Filing Rules
Appeal rights depend entirely on timelines. Each payer sets its own deadline. Missing it ends the conversation immediately.
Commercial payers usually allow between 90 and 180 days from the payment date. Medicare has structured appeal levels with strict timelines. Medicaid timelines vary by state and managed care organization.
Practices should never wait for month-end or quarter-end reviews. The underpayment review should occur within weeks of the payment posting. Early action preserves appeal rights.
Many recoverable underpayments are lost simply because they are discovered too late.
Medicare and Commercial Appeal Levels
Under Medicare, underpayment disputes follow a structured multi-level appeal process, beginning with redetermination and progressing through reconsideration and administrative law judge review if necessary.
Commercial payers often follow internal reconsideration and formal appeal stages. Understanding these levels strengthens recovery efforts and protects appeal rights.
CPT Codes Commonly Affected by Underpayments in Behavioral Health
Certain behavioral health CPT codes are more vulnerable to underpayments:
- 90834 – 45-minute psychotherapy
- 90837 – 60-minute psychotherapy
- 90853 – Group therapy
- 90839/90840 – Crisis psychotherapy
- 99213–99215 – Psychiatry E/M services
- 90792 – Psychiatric diagnostic evaluation
Time-based downgrades and add-on misprocessing frequently impact these services.
How to Appeal Underpayments in Behavioral Health Claims
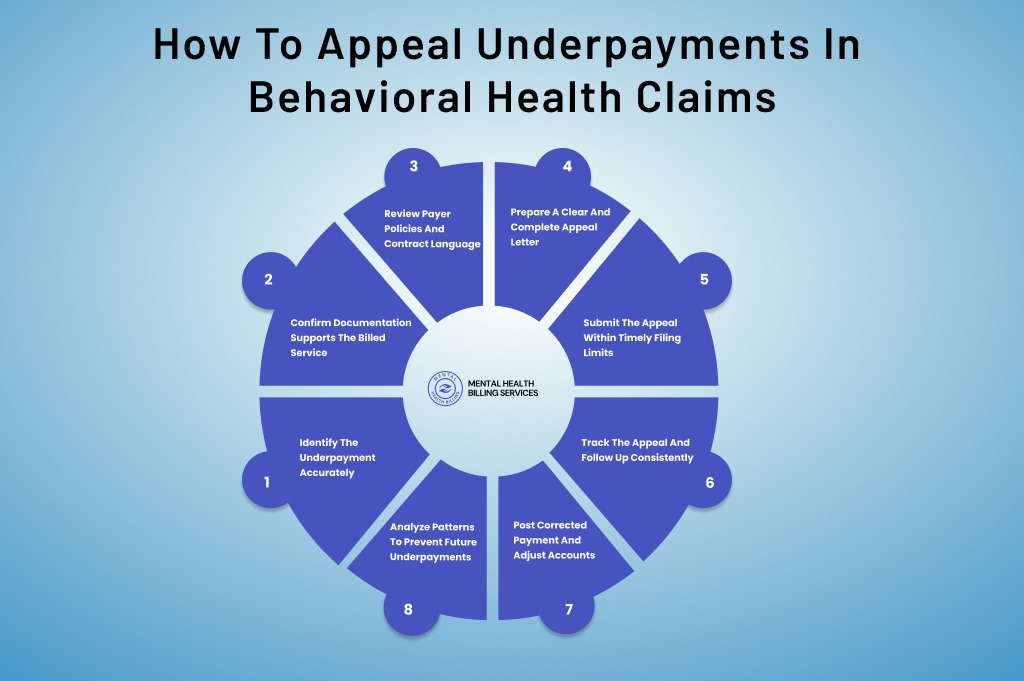
Appealing underpayments in behavioral health requires structure, timing, and persistence. The process is not complicated, but it demands consistency. When followed correctly, it recovers revenue that was already earned. Many practices fail here because they rush or skip steps. A step-by-step approach keeps the process clean and compliant.
Identify the Underpayment Accurately
The process starts with detection. A claim must be reviewed after payment posts. Do not assume paid means correct. Compare the paid amount on the EOB or ERA to the contracted allowed amount. This step requires access to payer contracts and current fee schedules. Behavioral health claims are especially vulnerable to time-based downgrades and stripped add-on codes. Look closely at therapy duration, crisis services, and telehealth claims. If the allowed amount does not match the contract, the claim qualifies for appeal.
Confirm Documentation Supports the Billed Service
Before appealing, confirm the clinical record fully supports the code billed. Time must be clearly documented for therapy and crisis services. Medical necessity must be evident. Provider credentials must align with payer requirements. If the documentation is weak, the appeal will fail. Appeals should proceed only when the service is defensible. Clean documentation strengthens your position and speeds resolution.
Review Payer Policies and Contract Language
Each appeal must be grounded in payer rules. Review the payer’s behavioral health policy, billing manual, and fee schedule. Identify where the payer processed the claim incorrectly. This may involve misapplying time thresholds, ignoring modifiers, or using an outdated rate. Referencing payer policy language increases approval rates. It shows that the appeal is not opinion-based. It is rule-based.
Prepare a Clear and Complete Appeal Letter
The appeal letter should be direct and factual. Include the claim number, date of service, CPT codes billed, and amount paid. Clearly state the expected allowed amount based on the contract or policy. Explain the discrepancy in simple language. Attach supporting documents, including the EOB, session notes, and relevant contract pages. Avoid emotional language. Professional clarity wins appeals.
Submit the Appeal Within Timely Filing Limits
Timelines matter. Commercial payers often allow 90 to 180 days from the payment date. Medicare and Medicaid have structured deadlines. Submit the appeal as soon as the underpayment is identified. Late submissions are denied automatically. Track submission dates carefully to protect appeal rights.
Track the Appeal and Follow Up Consistently
Submitting the appeal is not the end. Follow-up drives results. Log each appeal with a reference number and expected response date. Follow up every 30 days if no response is received. Many underpayment appeals require multiple touches before resolution. Persistence increases recovery rates significantly.
Post Corrected Payment and Adjust Accounts
Once the payer reprocesses the claim, review the corrected EOB. Confirm the allowed amount matches the contract. Post adjustments accurately. If payment is still incorrect, escalate to the next appeal level if available. Do not close the account until it balances correctly.
Analyze Patterns to Prevent Future Underpayments
Every appeal provides insight. Track which codes, payers, and scenarios underpay most often. Use this data to improve coding, documentation, and payer communication. Prevention reduces future workload and protects revenue.
Preventing Future Behavioral Health Underpayments
Recovering underpayments matters. Preventing them protects long-term revenue.
Behavioral health underpayments often follow predictable patterns. The same CPT codes get downgraded. The same modifiers are misprocessed. Telehealth logic is applied inconsistently. Identifying these trends early prevents recurring revenue loss.
Proactive contract monitoring is the foundation. Maintain updated payer fee schedules and compare allowed amounts regularly. Behavioral health reimbursement rates change more often than most practices realize. Without routine verification, outdated rates can silently reduce collections.
Front-end accuracy is equally critical. Eligibility verification should confirm not just coverage, but reimbursement structure and provider tiering. Many underpayments stem from credential-level rate mismatches that go unnoticed for months.
Clear, standardized documentation reduces time-based downgrades. Therapy notes must reflect total session minutes, medical necessity, and correct linkage of crisis or add-on codes. Consistency strengthens both initial claims and future appeals.
Regular modifier and telehealth audits also prevent repeat errors. Small configuration issues in billing systems can affect hundreds of claims before detection.
Preventing underpayments is not about constant appeals. It is about building structured behavioral health revenue cycle oversight that identifies discrepancies early and corrects them before revenue is lost.
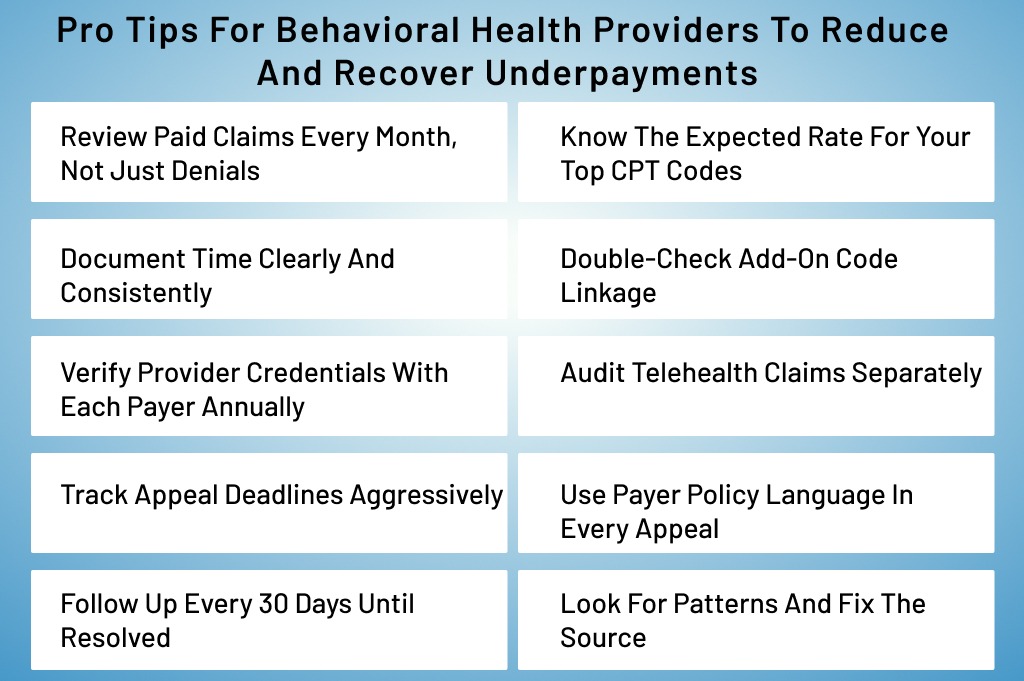
Pro Tips for Behavioral Health Providers to Reduce and Recover Underpayments
Behavioral health providers can protect revenue by becoming more involved in the billing process, even if billing is outsourced. You do not need to manage claims daily, but you should understand how your services are reimbursed. Knowing your common CPT codes and expected reimbursement ranges helps you recognize when something feels off. Awareness is the first layer of defense.
- Review paid claims every month, not just denials: Pull a simple paid-claims report and compare allowed amounts to your contract rates. Focus on high-volume CPT codes first. This habit alone catches most underpayments early.
- Know the expected rate for your top CPT codes: Keep a reference sheet with average allowed amounts by payer for common therapy, psychiatry, and crisis codes. When a payment looks low, you will spot it immediately.
- Document time clearly and consistently: Always include total session time in minutes for time-based services. Place it in the same spot in every note. Clear time documentation prevents code downgrades and strengthens appeals.
- Double-check add-on code linkage: Ensure crisis add-ons and prolonged service codes are correctly linked to the primary CPT. Review EOBs to confirm add-ons were not stripped or paid at zero.
- Verify provider credentials with each payer annually: Confirm that psychiatrists, psychologists, and therapists are loaded correctly. Credentialing errors often cause silent rate reductions across multiple claims.
- Audit telehealth claims separately: Review the place of service and modifiers regularly. Telehealth underpayments often stem from small setup errors that repeat across many claims.
- Track appeal deadlines aggressively: Create a simple tracker with payment date, appeal deadline, and submission date. Missing a deadline means permanent revenue loss.
- Use payer policy language in every appeal: Reference the payer’s own billing manual or contract terms. Appeals grounded in payer rules resolve faster and succeed more often.
- Follow up every 30 days until resolved: Do not assume no news is good news. Many underpayment appeals require multiple follow-ups before reprocessing happens.
- Look for patterns and fix the source: Track which payers and codes underpay most often. Adjust workflows, documentation, or billing rules to prevent repeat errors.
Conclusion
Underpayments are one of the most costly and overlooked problems in behavioral health billing. They do not announce themselves. They quietly reduce revenue while practices stay busy and providers work harder.
Appealing underpayments is not about chasing money. It is about claiming what was already earned. When done correctly, the process is compliant, professional, and effective.
Behavioral health practices that ignore underpayments struggle with cash flow, distorted financial data, and limited growth. Practices that address them operate with clarity and confidence.
By understanding why underpayments happen, identifying them early, and following a structured appeal process, providers protect their revenue without increasing patient volume.



